When Your Child Has Pulmonary Stenosis (PS)
The heart is divided into 4 chambers. The 2 upper chambers are called atria. The 2 lower chambers are called ventricles. The heart contains 4 valves. The valves open and close to keep blood flowing forward through the heart. The pulmonary valve is between the right ventricle and the pulmonary artery. It normally has 3 leaflets that open and close to allow blood through. It controls the flow of blood from the heart to the lungs. Pulmonary stenosis (PS) is when this valve doesn’t open all the way. It can also occur when the area above or below the valve is too narrow. As a result, blood flow to the lungs is blocked. If not treated, this condition can lead to some heart problems over time. But treatment can often be done.
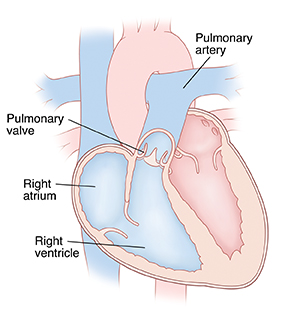 |
| Inside view of a normal heart. |
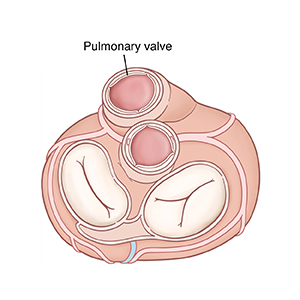 |
| Top view of heart. |
Types of pulmonary stenosis
PS comes in different types. They are:
-
Supravalvar. This is when blockage occurs just above the valve. The pulmonary artery may be too narrow.
-
Valvar. This is when blockage occurs at the valve. The leaflets may be too thick or are stuck together.
-
Subvalvar. This is when blockage occurs below the valve. The area below the valve may be too narrow.
-
Peripheral. This is when the narrowing is further along in the pulmonary artery. It may occur in 1 or both pulmonary arteries and in multiple places. The benign type can be found during a well child exam. It doesn't need treatment.
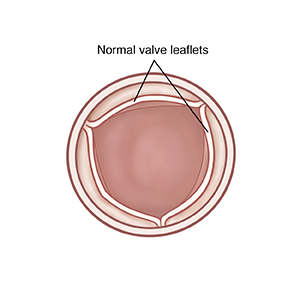 |
| An open normal pulmonary valve (view from above). |
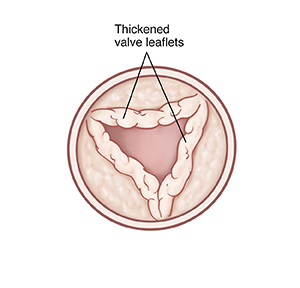 |
| An open pulmonary valve with stenosis. |
What causes pulmonary stenosis?
PS is a common congenital heart defect. It occurs in about 10% of people with congenital heart disease. It’s a problem with the structure of the heart that your child was born with. It can occur by itself. Or it can be part of a more complex set of defects. The exact cause is unknown. But most cases seem to occur by chance. Having a family history of heart defects can be a risk factor.
Why is pulmonary stenosis a problem?
PS forces the right ventricle to work harder to pump blood through the pulmonary valve into the pulmonary artery to reach the lungs. This causes the right ventricle to thicken (hypertrophy) and get larger. Over time, the right ventricle can become so overworked that it no longer pumps blood well. This condition is known as heart failure (HF).
Children with valve problems such as PS may be at risk of an infection of the heart’s inner lining or valves. This is called infective endocarditis.
The thickening of the right ventricle may increase your child's risk for abnormal heart rhythms or heartbeats (arrhythmias).
What are the symptoms of pulmonary stenosis?
Most children with an isolated PS will not have symptoms. The murmur may be heard during childhood as part of a well child exam or another visit. Children with mild or moderate PS often have no symptoms. Severe stenosis may be diagnosed on prenatal ultrasound. Children with severe or critical PS will often have symptoms. These can include:
-
Trouble breathing
-
Fast breathing
-
Trouble feeding (in babies)
-
Poor weight gain (in babies)
-
Blue tint to skin, lips, and nails due to lack of oxygen in the blood (cyanosis)
How is pulmonary stenosis diagnosed?
During a physical exam, your child's healthcare provider checks for signs of a heart problem, such as a heart murmur. This is an extra noise caused when blood doesn’t flow smoothly through the heart. If a heart problem is suspected, your child will be referred to a pediatric cardiologist. This is a healthcare provider who diagnoses and treats heart problems in children. Pulmonary stenosis may happen on its own, or it may be the result of several different problems. Your child may have tests, such as:
-
Chest X-ray. X-rays are used to take a picture of the heart and lungs.
-
Low-pulse oximetry. This test shows low oxygen levels before cyanosis develops.
-
Electrocardiogram (ECG). This test records the electrical activity of the heart.
-
Echocardiogram (echo). Sound waves (ultrasound) are used to create pictures of the heart and look for structural defects.
How is pulmonary stenosis treated?
Mild or moderate PS usually needs no treatment. Your child should have regular visits with a cardiologist. This is to make sure that narrowing of the valve doesn’t get worse over time.
Severe or critical PS needs treatment. Your child may be given a medicine for a time to keep the ductus arteriosus open. This lets blood flow to the pulmonary artery and lungs from the aorta, bypassing the blocked area. The main treatment for PS is a procedure called balloon valvuloplasty. This procedure is described below. In some cases, open heart surgery to repair or replace the valve is also a choice. The cardiologist will tell you more about heart surgery if it’s needed. Surgery is the treatment of choice for subvalvar and supravalvar PS.
What happens during balloon valvuloplasty?
Balloon valvuloplasty is a procedure done in the heart using a thin, flexible tube called a catheter. It’s done by a cardiologist who has special training to use catheters to treat heart problems (cardiac catheterization). The procedure lasts about 2 to 4 hours. It takes place in a catheterization laboratory (cath lab). You’ll stay in the waiting room during the procedure.
-
Before the procedure. You’ll be told to keep your child from eating or drinking anything for a certain amount of time before the procedure. Follow these directions carefully.
-
During the procedure. Your child is given medicine (sedative or anesthesia). This is to help them relax and not feel discomfort or pain during the procedure. A breathing tube may be placed in your child’s windpipe (trachea) during this time. Devices watch your child’s heart rate, blood pressure, and oxygen levels. The catheter insertion site in the groin is cleaned and numbed. Then the catheter is inserted into a blood vessel in the groin. With the help of live X-rays, the catheter is advanced up through this blood vessel into the heart. Contrast dye is usually injected through the catheter. The dye allows the inside of the heart to be seen on X-rays. A small balloon at the end of the catheter is inflated 1 or more times within the pulmonary valve. This forces the valve leaflets to open. The catheter and balloon are then removed.
-
After the procedure. Your child is taken to a recovery room. You can stay with your child during much of this time. It may take 1 to 4 hours for sedative medicines to wear off. Pressure is applied to the catheter insertion site to limit bleeding. A healthcare provider will tell you how long your child needs to lie down and keep the insertion site still. Your child is cared for and watched until they can leave the hospital. Your child will likely need to stay overnight in the hospital.
What are possible complications of balloon valvuloplasty?
Risks and possible complications of balloon valvuloplasty include:
-
Reaction to contrast dye
-
Reaction to sedative or anesthesia
-
Pain, swelling, redness, bleeding, or fluid leaking from the catheter insertion site
-
Leakage of blood through the pulmonary valve back into the right ventricle
-
Abnormal heart rhythm
-
The need for more treatment to repair or replace the valve
-
Injury to the heart or a blood vessel
In general, complications after balloon valvuloplasty are extremely rare.
When to call the healthcare provider
Call 911
-
Breathing difficulty, shortness of breath, or chest pain
-
Fainting or unresponsiveness
-
An irregular heartbeat
Call the healthcare provider right away if your child has any of these:
-
Pain, swelling, warmth, redness, bleeding, or fluid leaking from the catheter insertion site that gets worse
-
Feveras directed by your healthcare provider
-
Lightheadedness
-
Arm or leg turns blue or feels cold
What are the long-term concerns?
All treatment choices for PS are done to relieve symptoms. This means that the pulmonary valve is not repaired. It will always be somewhat abnormal. Your child may have problems with the valve again in the future.
After treatment, most children with PS can be as active as other children. They will need regular follow-up visits with a cardiologist. This is to make sure the valve doesn’t become blocked again or have too much leakage. Your child may need fewer follow-up visits as they grow older.