Prostate Cancer: Early Detection
Screening means checking for a health problem before a person has symptoms. This can sometimes help find diseases, like certain cancers, early. This can lead to early treatment. Finding and treating cancer early, when it's small and hasn't spread, may improve the chance that treatment will work better.
But it's still not clear exactly how helpful screening is for prostate cancer. Learning more about prostate cancer screening and the risks and benefits of it can help you decide if it's right for you.
Screening tests for prostate cancer
Two screening tests can be used to check for prostate cancer:
-
PSA blood test. This test looks at the level of prostate-specific antigen (PSA) in the blood. PSA is a protein made by prostate cells. A high level means it's more likely that a person has prostate cancer. This test can be done alone or with a digital rectal exam.
-
Digital rectal exam (DRE). In this exam, the healthcare provider puts a lubricated, gloved finger into the rectum to check the size of the prostate and feel the surface through the bowel wall for hard lumps or abnormal areas. Only part of the prostate surface can be felt during the exam. A DRE is best performed with a PSA blood test.
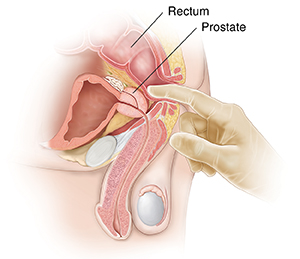 |
| The DRE takes just a few seconds. |
Abnormal results on these screening tests can mean that a person might have prostate cancer, but these tests can’t diagnose prostate cancer. A prostate biopsy is needed to be sure. A biopsy is when tiny pieces of tissue are taken out and tested in a lab.
Why prostate cancer screening is controversial
Not all healthcare providers agree that prostate cancer screening is useful. This is because:
-
PSA test results aren't always right. In some cases, the PSA test can have false-positive or false-negative results. A false positive means that test results show that a person may have cancer when they don't. This can lead to more tests, which can lead to stress and possible harm from the tests. A false negative means that test results don’t show cancer when a person has it. This can mean you don't get the extra tests or treatment you need.
-
Finding prostate cancer early may not be helpful. Even if screening does help find cancer early, prostate cancer often grows slowly and mostly affects older adults. This means that finding it early may not lead to a longer life. Many people with prostate cancer die years later of other causes without having symptoms or being treated for their prostate cancer.
But healthcare providers can’t always tell which cancers are likely to grow fast and need to be treated. And even if a cancer is slow-growing, a person may not be OK with living with cancer. They may want it treated. Treatment for prostate cancer can have very serious side effects, such as erection problems and lack of urine control (incontinence).
Research in progress
It’s not yet clear if the benefits of screening for prostate cancer are greater than the possible harms. Research studies have found that prostate cancer screening can find more cancers. But it's still not clear if screening saves enough lives to outweigh the harm treatment can cause.
Researchers are looking for better ways to know:
-
Which prostate cancers need to be treated early
-
Which prostate cancers can be safely watched over time instead
-
The ideal age to start and stop screening
-
The ideal frequency of testing
-
How to best screen high-risk people
At this time there are no standard tests that give this kind of information.
What expert groups recommend
Most expert medical groups agree that routine prostate cancer screening should not be done for all men. But the advice varies between groups. For example:
-
U.S. Preventive Services Task Force says that people ages 55 to 69 should talk with their healthcare providers about the possible benefits and harms of screening in order to make an informed decision.
-
American Urological Association says that people should talk with their healthcare providers about the pros and cons of screening. They suggest that people ages 50 to 69 at average risk for prostate cancer should be given the choice to have prostate screening. They suggest that people may begin screening as young as ages 45 to 50. Those at higher risk could have this choice earlier.
-
National Comprehensive Cancer Network says that people talk with their healthcare providers about the pros and cons of screening starting at age 45. Those at high risk should have this talk at age 40.
-
American Society of Clinical Oncology says that people expected to live at least 10 years should talk with their healthcare providers about whether or not screening is right for them.
-
American Cancer Society (ACS) says that people should talk with their healthcare providers about the pros and cons of screening. They advise having this talk at age 50 for those at average risk who are expected to live for 10 years or more. People who are black of African ancestry or who have a father or brother (first-degree relative) diagnosed with prostate cancer before age 65 are at high risk and should have this talk at age 45. ACS advises people to discuss screening at age 40 if they are at even higher risk. This means having more than one first-degree relative diagnosed before age 65.
Making a decision
All the medical expert groups advise that people talk with their healthcare providers to make an informed decision about screening. If you're thinking about being screened, talk with your healthcare provider about:
-
Your personal risk of prostate cancer based on your age, race, and family history
-
What the screening test results can and can’t tell you
-
What the next steps would be if the test results show you might have prostate cancer
-
What your choices would be for treating or not treating right away
-
What the treatment choices are if you were to have treatment, including the benefits and possible harms of different treatments
Online Medical Reviewer:
Jessica Gotwals RN BSN MPH
Online Medical Reviewer:
Susan K. Dempsey-Walls APRN
Online Medical Reviewer:
Todd Gersten MD
Date Last Reviewed:
8/1/2023
© 2024 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare provider's instructions.